Spinal Deformity Correction
Surgical realignment of an abnormally curved spine — through instrumentation, fusion, and where required, osteotomy — to restore functional balance and relieve neural compression.
Overview
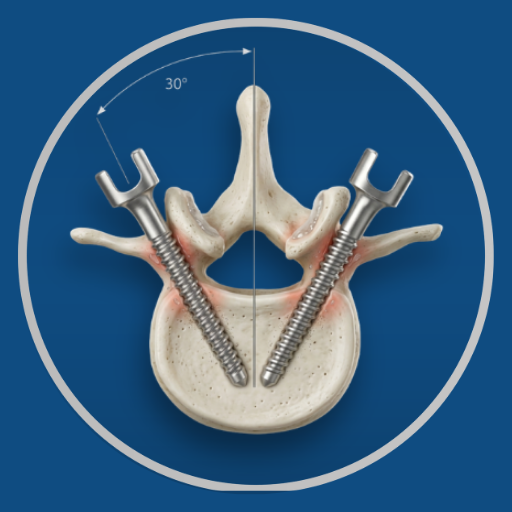
Spinal deformity correction is among the most technically demanding procedures in spine surgery. It involves the placement of multiple spinal screws and rods across the deformed segments, correction of the curve through rod contouring and intraoperative positioning, fusion of the corrected levels, and in selected cases, osteotomies — deliberate controlled cuts through vertebrae to allow angular correction that cannot be achieved through positioning alone. The goal is a spine that is balanced in both the coronal and sagittal planes — one that the patient can stand upright with, bear load on symmetrically, and maintain long-term.
Before Surgery
Deformity correction surgery requires extensive pre-operative planning. Full-length standing X-rays with sagittal and coronal balance measurements, MRI for neural assessment, CT for bony anatomy and navigation planning, pulmonary function testing where thoracic deformity is involved, and medical optimisation for what is typically a longer procedure with greater physiological demand. Nutritional assessment and correction of any bone health deficiencies are addressed before surgery. A detailed pre-operative discussion covers the planned correction, expected outcomes, and the specific risks of the procedure.
During Surgery
Performed under general anaesthesia with intraoperative neurophysiological monitoring (IONM) — continuous monitoring of the spinal cord and nerve root function throughout the procedure to detect any change that warrants immediate surgical response. The Medtronic O-arm and StealthStation navigation system provide real-time three-dimensional imaging and instrument guidance for screw placement in anatomy that is often significantly distorted from normal by the deformity. The correction is achieved progressively through rod placement, compression and distraction manoeuvres, and osteotomies where planned. Duration is 4–8 hours depending on the number of levels and complexity of correction required.
After Surgery
Post-operative care is in a monitored setting initially. Hospital stay of 5–7 days. Pain management is structured and progressive. Early mobilisation — typically day 1 or 2 post-operatively — is important for respiratory function and venous circulation. Physiotherapy begins in hospital and continues through the recovery period.
Recovery
Full recovery from deformity correction is measured in months. Restrictions on heavy loading, bending, and twisting apply for the first 3–4 months while the fusion consolidates. Desk work is typically possible within 8–12 weeks. Physical activity returns progressively from 3–6 months, guided by clinical assessment and imaging. Long-term outcomes in appropriately selected patients — measured by pain reduction, functional improvement, and maintained correction on follow-up X-rays — are durable.
Dr. Viswanath's Approach
Deformity correction is a clinical focus of this practice. Navigation-assisted technique using the Medtronic O-arm and StealthStation system is used routinely — in a setting where anatomy is distorted and screw trajectories must be planned and executed with precision, navigation is not optional. Intraoperative neurophysiological monitoring is used for all major deformity correction procedures. The surgical plan is developed from detailed pre-operative imaging analysis and is discussed thoroughly with the patient before any procedure is scheduled.
Medical Disclaimer: This information is provided for educational purposes only and does not constitute medical advice.