Spinal Stenosis
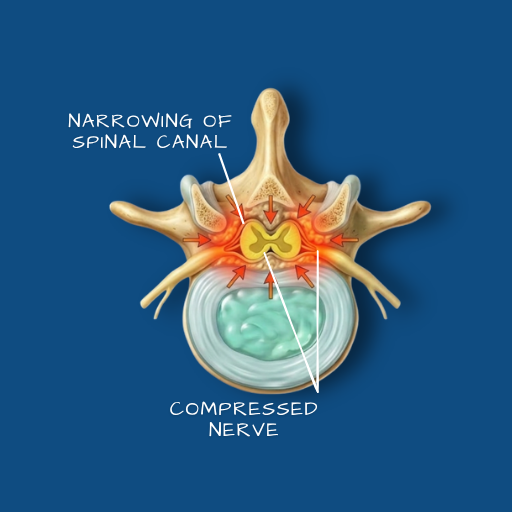
A narrowing of the spinal canal that places pressure on the nerves passing through it — causing pain, weakness, and reduced tolerance for walking or standing.
Overview
The spinal canal is the bony channel that runs the length of the spine, housing the spinal cord and the nerve roots that branch from it. Spinal stenosis refers to a narrowing of this canal — or of the smaller openings through which individual nerve roots exit — that creates pressure on the neural structures within. It is most common in the lumbar spine, though cervical stenosis (in the neck) is also encountered and carries additional considerations related to spinal cord involvement. Stenosis is predominantly a condition of gradual onset, developing over years rather than weeks. It is most frequently seen in patients over 50, though it can occur earlier in those with structural or developmental predispositions.
Causes
The most common cause is degenerative change — the cumulative effect of age-related wear on the discs, facet joints, and ligaments that surround the spinal canal. As discs lose height, the joints and ligaments that compensate for that loss can thicken and encroach on the available space within the canal. Bone spurs (osteophytes) may form on the vertebral edges, further reducing the canal’s cross-sectional area. In some patients, a herniated disc contributes to the narrowing. Less commonly, stenosis has a structural or congenital basis — a canal that was inherently narrower than average before any degeneration began.
Symptoms
The characteristic symptom of lumbar spinal stenosis is neurogenic claudication — a heaviness, cramping, or aching in the legs that appears after walking or standing for a period of time and is relieved by sitting or bending forward. Patients often describe being able to walk a limited distance before needing to rest, and finding that leaning on a shopping trolley or walking uphill (which flexes the spine and opens the canal slightly) eases their symptoms. Back pain may also be present, but the leg symptoms are often more prominent. In cervical stenosis, the presentation may include arm symptoms, difficulty with fine motor tasks, gait disturbance, or, in more severe cases, signs of spinal cord compression.
Diagnosis
The clinical history — particularly the pattern of symptom onset, relief, and functional limitation — is highly informative for stenosis diagnosis. MRI is the definitive imaging study, providing detail on the degree of canal narrowing, the level or levels involved, and the condition of the discs and facet joints. CT myelography may be used as an alternative or complement to MRI in specific situations. Standing X-rays are useful for assessing spinal alignment and any dynamic instability that may be contributing to the stenosis.
Conservative Care
Physiotherapy for spinal stenosis focuses on spinal flexion exercises — positions and movements that open the canal and temporarily relieve nerve pressure — alongside core strengthening to provide better spinal support. Epidural steroid injections can provide meaningful, though typically temporary, relief of the nerve-related symptoms and are sometimes used to facilitate engagement with physiotherapy. Activity modification — understanding and working within the patient’s symptomatic limits — forms part of the management plan. Conservative care is appropriate for patients with manageable symptoms and no neurological deterioration. Its role is to improve quality of life and delay or avoid surgical intervention where possible.
Surgical Indications
Surgical intervention is considered when symptoms are significantly limiting daily function, when conservative care has not produced adequate relief, or when there is evidence of progressive neurological impairment. Patients who cannot walk a meaningful distance, who are waking at night with symptoms, or who are unable to manage their daily activities despite non-surgical care are typically the surgical candidates. The presence of spinal cord involvement in cervical stenosis lowers the threshold for intervention, as the consequences of delayed treatment can be more significant.
Surgical Approach
The most common surgical procedure for lumbar spinal stenosis is a laminectomy — removal of the bony arch (lamina) at the back of the vertebra to create more space within the canal. This may be performed at a single level or across multiple levels depending on the extent of the stenosis. Where the stenosis is accompanied by spinal instability or spondylolisthesis, a fusion procedure may be added to stabilise the affected segment. Minimally invasive approaches are used where the clinical picture permits, reducing soft tissue disruption and aiding recovery. The Medtronic O-arm and StealthStation system provide intraoperative guidance in procedures involving instrumentation, ensuring accurate placement and reducing the risk of positional complications.
Recovery
Recovery from lumbar decompression surgery depends on the extent of the procedure. Single-level laminectomies generally allow discharge within two to three days, with a gradual return to activity over six to twelve weeks. Fusion procedures involve a longer recovery, with more structured restrictions in the early weeks and physiotherapy playing a greater role in rebuilding strength and movement. Neurological symptoms — particularly leg heaviness and cramping — typically improve progressively over weeks to months. Full functional recovery in complex cases may take up to six months or longer, and realistic expectations are discussed with each patient before any procedure is planned.
If walking distance, leg symptoms, or daily function have become limited by spinal pain, a clinical evaluation is the appropriate first step.