Laminectomy
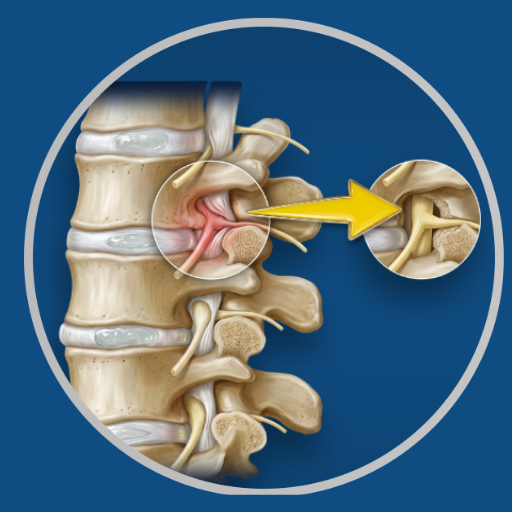
Removal of the bony arch (lamina) at the back of one or more vertebrae to create more space within the spinal canal and relieve pressure on the spinal cord or nerve roots.
Overview
Laminectomy is the most commonly performed decompression procedure for lumbar spinal stenosis. The lamina — the flat bony plate that forms the posterior wall of the spinal canal — is removed at the affected level or levels, directly enlarging the canal and relieving the pressure on the neural structures within it. It may be performed alone for stenosis without instability, or combined with fusion where there is associated spondylolisthesis or significant segmental instability.
Before Surgery
MRI confirming the level and extent of stenosis. Standing X-rays to assess alignment and any instability. Medical clearance. Discussion of whether fusion will be required alongside decompression.
During Surgery
General anaesthesia. Prone positioning. A midline incision over the affected levels. The paraspinal muscles are retracted to expose the lamina. The lamina and the thickened ligamentum flavum are removed carefully, decompressing the nerve roots. The facet joints are partially preserved where possible to maintain stability. Microsurgical technique or magnification is used to protect neural structures during decompression. The Medtronic StealthStation system is used where instrumentation is added. Duration: 1–3 hours depending on levels.
After Surgery
Hospital stay is 2–3 days for single-level decompression. Pain at the wound site managed with medication. Mobilisation begins day 1.
Recovery
Return to desk work within 4–6 weeks. Return to physical activity within 8–12 weeks. Physiotherapy begins 2–4 weeks post-operatively. Neurogenic claudication — the leg heaviness with walking that characterises stenosis — typically improves progressively over weeks to months.
Dr. Viswanath's Approach
Laminectomy is performed with careful attention to the extent of bony removal — enough to achieve adequate decompression, while preserving facet joint integrity to avoid creating instability that then requires fusion. Where instability is identified preoperatively or intraoperatively, fusion is planned and performed at the same sitting rather than as a secondary procedure.
Medical Disclaimer: This information is provided for educational purposes only and does not constitute medical advice.