Spinal Deformity / Scoliosis
Abnormal curvature of the spine — in the coronal, sagittal, or axial plane — that may affect posture, balance, pain, and in advanced cases, respiratory or neurological function.
Overview
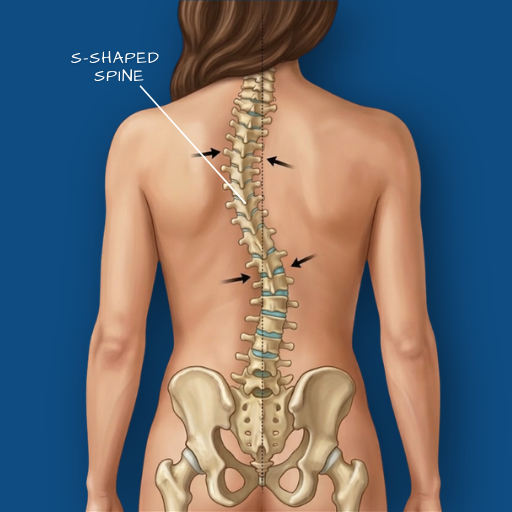
The spine viewed from behind should be straight. Viewed from the side, it carries natural curves — a forward curve in the neck and lower back (lordosis), and a backward curve in the thoracic region (kyphosis). Spinal deformity refers to abnormal curvature in any of these planes. Scoliosis — a lateral (sideways) curvature — is the most commonly encountered deformity. It can occur as an isolated structural abnormality (idiopathic scoliosis, most common in adolescents) or develop secondary to degenerative changes in adulthood (degenerative scoliosis), neurological conditions, or prior spinal surgery. Sagittal deformity — a loss of the normal side-profile alignment — is increasingly recognised as a significant contributor to pain and functional disability in adult patients, particularly those with long-standing degenerative disease. Deformity correction is one of Dr. Viswanath’s areas of focused surgical expertise.
Causes
In adolescents, idiopathic scoliosis has no clearly identified single cause — it is thought to involve a combination of genetic predisposition and growth-related spinal asymmetry. In adults, degenerative scoliosis develops as asymmetric disc and facet joint degeneration causes the spine to curve laterally over time. Other causes include neuromuscular conditions (cerebral palsy, muscular dystrophy), congenital vertebral malformations, prior spinal surgery that has altered load distribution, and metabolic bone disease. Sagittal imbalance — the loss of normal lumbar lordosis — commonly develops following multi-level degenerative disease, following certain spinal fusions, or as a consequence of long-standing flat-back posture.
Symptoms
Symptoms depend on the type, severity, and location of the deformity. Mild scoliosis may be entirely asymptomatic and identified incidentally on imaging. Moderate to severe curves can produce back pain from asymmetric loading, fatigue from postural compensation, and visible changes in posture — uneven shoulder height, a prominent rib on one side, or a visible lateral list. Sagittal deformity often presents as an inability to stand straight without significant effort, with compensatory flexion at the hips and knees. In more severe or progressive deformities, nerve root compression, spinal cord compression, and in thoracic deformities, reduced respiratory capacity can occur. The relationship between curve severity (measured in degrees on X-ray — the Cobb angle) and symptoms is not linear — clinical assessment considers both.
Diagnosis
Full-length standing spinal X-rays (from head to pelvis) are the primary and most important imaging study for deformity assessment, capturing the true three-dimensional alignment of the spine under load. The Cobb angle — the standard measurement of scoliotic curve magnitude — is calculated from these X-rays. Flexibility films (taken in bending positions) help assess the degree to which a curve is structural versus flexible, which directly informs surgical planning. MRI provides information on disc health, nerve compression, and cord involvement. CT scanning is used for detailed bony anatomy in complex deformity cases. Pulmonary function testing may be requested where thoracic deformity is significant.
Conservative Care
For mild scoliosis without symptoms, observation with periodic X-ray monitoring is appropriate — the focus is on identifying any progression of the curve over time. For symptomatic deformity without severe structural compromise, physiotherapy addressing core strength, postural awareness, and movement quality can meaningfully improve pain and functional capacity. Bracing is used in adolescent idiopathic scoliosis to slow curve progression during growth — it is not indicated for adult degenerative deformity. Pain management, including medications and injections, can provide symptomatic relief in degenerative cases. Conservative management is the appropriate framework for patients with manageable symptoms, stable curves, and no neurological compromise.
Surgical Indications
Surgery for spinal deformity is considered when conservative management has not provided adequate relief and the patient’s quality of life is significantly impaired, when the curve is progressive and reaches a degree likely to continue worsening, when neurological compromise is present, or when the deformity is causing cardiorespiratory limitation in thoracic cases. Sagittal imbalance that prevents a patient from standing upright and functioning adequately is a strong indication for corrective surgery. The decision to operate is made carefully, as deformity surgery is technically demanding and carries a higher risk profile than decompression procedures — full patient understanding of the procedure and its implications is part of the pre-operative process.
Surgical Approach
Spinal deformity correction is Dr. Viswanath’s area of focused surgical expertise. The operative goal is to achieve a balanced, stable spine — correcting the deformity to a degree that restores functional alignment and relieves neural compression, while accounting for what is safely achievable given the patient’s age, bone quality, and overall health. Correction is achieved through a combination of segmental spinal instrumentation (pedicle screws and rods), fusion of the corrected segments, and in some cases osteotomies — controlled cuts through the vertebra to allow angular correction. The Medtronic O-arm and StealthStation navigation system are used routinely in deformity correction surgery, providing real-time three-dimensional guidance for screw placement in a setting where anatomy is often significantly distorted from normal. Minimally invasive techniques are used for selected cases, particularly in early or moderate adult degenerative deformity where a full open correction is not required.
Recovery
Recovery from deformity correction surgery is the most substantial of all spinal procedures, and realistic expectations are an essential part of the pre-operative discussion. Hospital stay is typically five to seven days. Early recovery involves structured mobility with restrictions, pain management, and the beginning of physiotherapy. The fusion and instrumentation take six to twelve months to consolidate fully, and restrictions on heavy loading and high-impact activity apply during this period. Patients typically return to light activity within eight to twelve weeks, desk work within six to ten weeks, and physical activity on a timeline guided by clinical and imaging progress. Long-term outcomes in appropriately selected patients — measured in pain reduction, improved posture, and functional gains — are meaningful and durable.
Spinal deformity evaluation requires specialist assessment and full-length standing imaging. If posture, pain, or functional capacity have become a concern, a consultation is the appropriate starting point.