Cervical Disc Disease
Disc-related conditions in the cervical spine (neck) that can produce neck pain, arm pain, numbness, or weakness, and in more advanced cases, signs of spinal cord involvement.
Overview
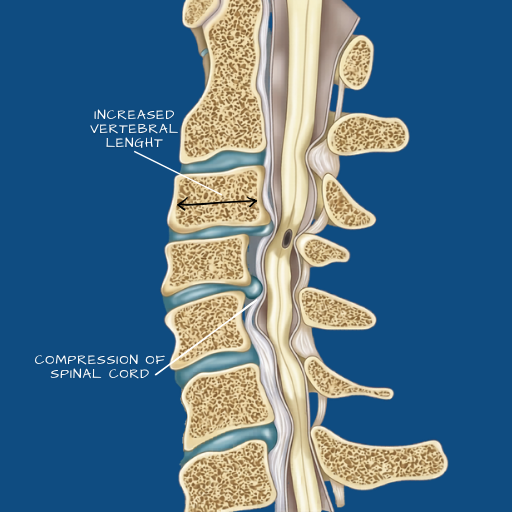
The cervical spine consists of seven vertebrae that support the head and allow the neck its range of movement. Between each vertebra sits an intervertebral disc — and like those in the lumbar spine, cervical discs are subject to degeneration, herniation, and the structural changes that accompany age and load. Cervical disc disease is a broad term that encompasses disc herniation in the neck, degenerative disc change at cervical levels, and the secondary structural changes — bone spurs, foraminal narrowing, and in more advanced cases, spinal canal narrowing — that result from long-standing degeneration. What makes cervical conditions clinically distinct from lumbar ones is their proximity to the spinal cord itself. Where lumbar nerve root compression causes leg symptoms, cervical cord compression (myelopathy) can affect coordination, hand function, gait, and bladder control — a clinical picture that requires careful evaluation and, in some cases, more urgent management.
Causes
Age-related disc degeneration is the most common underlying cause, with degenerative changes present in a significant proportion of adults over 40 even without symptoms. Cervical disc herniation — where inner disc material extrudes through a tear in the outer ring — can occur acutely with physical exertion or minor trauma, or develop gradually through cumulative loading. Sustained postures that load the cervical spine — extended screen use, desk work without ergonomic support, and occupations requiring overhead work or repetitive neck movement — are contributing factors. Structural narrowing of the foramina (the exit channels for nerve roots) can develop through a combination of disc height loss and bone spur formation, and may produce progressive nerve root symptoms without a discrete disc herniation.
Symptoms
Neck pain is the most common symptom, often described as a deep ache that may radiate across the shoulders or between the shoulder blades. Cervical radiculopathy — nerve root compression — produces pain, numbness, or tingling that radiates into one arm, following the distribution of the affected nerve root. Weakness in specific arm or hand muscle groups may accompany severe compression. Cervical myelopathy, caused by compression of the spinal cord itself, presents differently — patients may notice difficulty with fine motor tasks (buttoning a shirt, writing), a sense of heaviness or stiffness in the legs, an unsteady gait, or urgency with bladder or bowel function. Myelopathic symptoms should be evaluated promptly, as the window for preventing permanent neurological change is time-sensitive.
Diagnosis
MRI of the cervical spine is the primary diagnostic study, providing detail on disc condition, foraminal narrowing, cord compression, and any signal change within the spinal cord that indicates myelopathy. CT myelography may be used where MRI is contraindicated or where surgical planning requires additional bony detail. Neurological examination — assessing reflexes, sensory distribution, motor strength, and coordination — is essential for correlating imaging findings with clinical presentation. Electromyography (EMG) or nerve conduction studies may be requested where the clinical picture is complex or where a peripheral nerve problem needs to be distinguished from a cervical root problem.
Conservative Care
Cervical radiculopathy without myelopathy or progressive neurological deficit responds well to conservative management in many cases. Physiotherapy addressing cervical alignment, muscle strengthening, and neural mobilisation is the primary treatment. Selective nerve root injections can provide meaningful symptomatic relief and serve a diagnostic function — confirming the specific level responsible for the patient’s symptoms. Activity modification, ergonomic assessment, and the avoidance of sustained provocative postures form part of the plan. Conservative care is appropriate for patients with manageable symptoms and no evidence of cord involvement or progressive neurological change.
Surgical Indications
Surgical intervention is considered when conservative care has failed to provide adequate relief over an appropriate trial period, when neurological deficits are present and not improving, or when myelopathy is identified. The presence of spinal cord compression with clinical signs of myelopathy substantially lowers the threshold for intervention — the natural history of untreated cervical myelopathy is variable but includes a risk of stepwise neurological deterioration, and surgery offers the best chance of stabilising or reversing the deficit.
Surgical Approach
The two most common surgical approaches for cervical disc disease are anterior cervical discectomy and fusion (ACDF) and cervical disc replacement (arthroplasty). ACDF involves removing the affected disc through an incision at the front of the neck, decompressing the nerve root or spinal cord, and stabilising the segment with a cage and plate. It is the most established procedure for cervical radiculopathy and myelopathy, with a well-documented outcome record. Cervical disc replacement preserves motion at the treated level and is appropriate for selected patients — typically younger, with single- or two-level disease and no significant instability. The choice between the two procedures is based on the clinical picture, the imaging, and the patient’s age and activity level. Navigation-assisted technique is applied where anatomy or multi-level disease warrants additional intraoperative guidance.
Recovery
Recovery from ACDF is generally well-tolerated. Most patients are mobile within 24 hours and discharged within two to three days. A collar may be worn for a short period depending on the construct. Return to desk work is typically possible within four to six weeks. The fusion process takes three to six months to consolidate, and activities involving significant neck loading are restricted during this period. Cervical disc replacement has a similar early recovery profile. Neurological symptoms — arm pain, numbness — typically improve progressively over weeks to months as the nerve recovers from compression. Myelopathic symptoms may improve partially or fully following decompression, though the extent of recovery depends on the severity and duration of cord compression before surgery.
Neck pain, arm symptoms, or any change in hand coordination or walking should be evaluated rather than observed without assessment.