Cervical Disc Replacement
A motion-preserving alternative to cervical fusion — replacing a degenerated or herniated cervical disc with an artificial disc implant that maintains movement at the treated level.
Overview
Anterior cervical discectomy and fusion (ACDF) has long been the standard surgical treatment for cervical disc disease. Cervical disc replacement (CDR), also known as cervical arthroplasty, is a more recent alternative that achieves the same decompression of the nerve root or spinal cord while preserving motion at the treated level rather than fusing it. The theoretical advantage is reduced stress on the adjacent discs — a concern with fusion, which eliminates movement at one level and may accelerate degeneration at the levels above and below over time. Long-term data on CDR continue to accumulate, and outcomes are favourable in appropriately selected patients.
Before Surgery
CDR is appropriate for patients with single- or two-level cervical disc disease causing radiculopathy or mild myelopathy, without significant instability, ossification of the posterior longitudinal ligament, or severe facet joint degeneration. MRI and CT are required to confirm candidacy. Patients with active inflammatory arthritis or significant osteoporosis are generally not candidates.
During Surgery
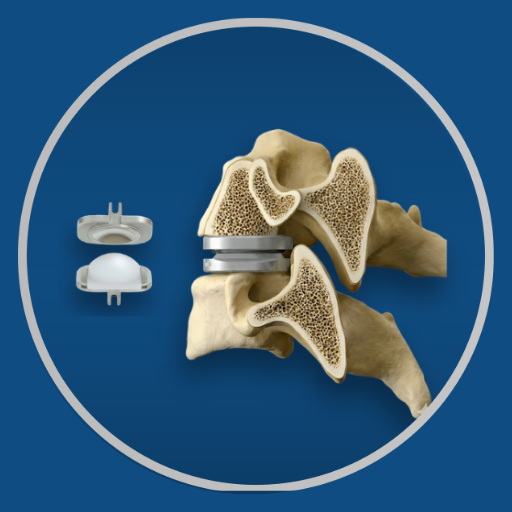
The approach is identical to ACDF — through a small incision at the front of the neck, the affected disc is removed and the nerve root or spinal cord is decompressed. Instead of a fusion cage and plate, an artificial disc prosthesis is implanted in the disc space, sized and positioned to restore disc height and allow the natural range of motion at that level. Duration is typically 1–2 hours.
After Surgery
Hospital stay of 1–2 days. A collar is typically not required or worn for a very short period. Pain at the incision site settles within a few days. Nerve symptom improvement follows the same trajectory as ACDF.
Recovery
Return to desk work within 3–4 weeks. Return to physical activity within 6–8 weeks, with cervical loading restrictions for 3 months while the implant integrates. The absence of a fusion means no bone graft consolidation timeline — recovery is typically faster than ACDF.
Dr. Viswanath's Approach
The choice between CDR and ACDF is made on a patient-specific basis, considering age, pathology level, imaging findings, and activity level. CDR is offered where the clinical picture supports it — it is not applied as a default, nor withheld from appropriate candidates. The same quality of decompression that guides ACDF applies equally to CDR.
Medical Disclaimer: This information is provided for educational purposes only and does not constitute medical advice.