Sciatica / Nerve Compression
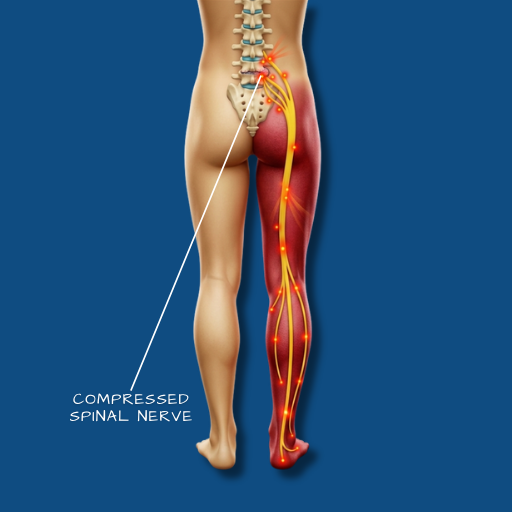
Pain, numbness, or weakness that originates in the lumbar spine and travels into the leg — following the path of the sciatic nerve or one of its contributing nerve roots.
Overview
Sciatica is not a diagnosis in itself — it is a symptom pattern. The term describes pain that radiates from the lower back or buttock into one leg, following the distribution of the sciatic nerve or one of the lumbar nerve roots that form it. It is caused by irritation or compression of a spinal nerve root, most commonly at the L4, L5, or S1 levels. The underlying cause is typically a disc herniation, spinal stenosis, spondylolisthesis, or in some cases a piriformis syndrome or other extra-spinal compression. Understanding the cause is essential for directing treatment correctly — the symptom pattern may look similar regardless of the underlying pathology, but the management pathway differs significantly depending on what is actually compressing the nerve.
Causes
The most common cause is a lumbar disc herniation at the L4–5 or L5–S1 level, where herniated disc material compresses the exiting nerve root. Spinal stenosis — narrowing of the canal or the nerve root exit channels (foramina) — produces a similar radiating pain pattern, typically brought on by walking or standing and relieved by sitting or bending forward. Spondylolisthesis, where one vertebra has shifted forward over another, can compress nerve roots at the affected level. Less commonly, sciatic-like symptoms are produced by piriformis syndrome — where the piriformis muscle in the buttock irritates the sciatic nerve directly — or by a tumour, infection, or other pathology. These less common causes are identified through careful clinical assessment and imaging.
Symptoms
The defining feature of sciatica is radiating pain — a sharp, burning, or electric sensation that travels from the lower back or buttock into the thigh, calf, or foot, on one side. The specific distribution of symptoms reflects which nerve root is compressed: L4 compression typically produces medial lower leg symptoms; L5 affects the outer calf and top of the foot; S1 involves the outer foot and sole. Numbness and tingling in the same distribution are common. Muscle weakness — foot drop (difficulty lifting the foot), calf weakness, or difficulty rising from a squat — indicates more significant nerve involvement. Symptoms that are worsened by sitting, coughing, or sneezing suggest a disc herniation as the cause. Symptoms relieved by sitting and worsened by walking suggest stenosis. Red flag symptoms — loss of bladder or bowel control, numbness in the saddle area (inner thighs and perineum), or rapidly progressive weakness in both legs — require immediate emergency evaluation for cauda equina syndrome.
Diagnosis
Clinical examination — including straight leg raise testing, neurological assessment of reflexes, sensation, and motor power in the lower limbs — provides the initial clinical picture and identifies the likely level and severity of nerve involvement. MRI of the lumbar spine is the definitive imaging study, identifying the cause and level of nerve compression. CT scanning may be used where bony detail is specifically required or where MRI is unavailable. Where the diagnosis is uncertain or multiple levels are involved, selective nerve root injections can serve both a therapeutic and a diagnostic function — confirming the responsible level when imaging and examination are not conclusive.
Conservative Care
The majority of sciatica episodes — particularly those caused by disc herniation — resolve or significantly improve with structured conservative management over six to twelve weeks. Physiotherapy addresses nerve mobility, lumbar stabilisation, and the postural and movement patterns that aggravate nerve irritation. Anti-inflammatory medications and nerve pain medications (such as gabapentinoids) are used to make the acute phase more manageable. Epidural steroid injections can provide significant relief during acute flare-ups and facilitate engagement with physiotherapy. Activity guidance — not bed rest, but the avoidance of specific aggravating postures and loads — is important in the early weeks. Conservative management is appropriate for all patients without progressive neurological deficit or red flag symptoms.
Surgical Indications
Surgery is considered when conservative care over an adequate trial period has not produced sufficient improvement, when the patient’s quality of life remains significantly impaired by persistent pain or functional limitation, or when neurological deficits — weakness, progressive numbness — are present and not resolving. Cauda equina syndrome, identified by its characteristic symptom cluster, is a surgical emergency requiring immediate decompression.
Surgical Approach
For sciatica caused by disc herniation, microdiscectomy is the procedure of choice — a minimally invasive operation in which the herniated disc fragment is removed through a small incision, directly relieving pressure on the affected nerve root. For sciatica caused by stenosis or spondylolisthesis, the appropriate procedure depends on the underlying pathology — decompression alone, or decompression combined with fusion where instability is present. The Medtronic StealthStation navigation system is used in procedures involving instrumentation, ensuring accurate placement and reducing operative risk. The goal in all cases is nerve decompression with the smallest necessary intervention.
Recovery
Following microdiscectomy for disc-related sciatica, leg pain relief is often experienced quickly — within days to weeks of surgery. Nerve symptoms (numbness, tingling) take longer to resolve as the nerve recovers from compression, and in some cases may persist for several months. Early mobilisation is encouraged, with activity restrictions in the first two to four weeks. Physiotherapy begins two to four weeks post-operatively and focuses on restoring movement, strength, and the postural habits that support long-term spinal health. Return to desk work is typically possible within four to six weeks. Full recovery and return to physical activity takes three to six months.
Leg pain originating from the spine is among the most treatable of spinal symptoms when evaluated and managed appropriately.