Sacroiliac Joint Dysfunction
Pain arising from the sacroiliac joint — the joint connecting the base of the spine to the pelvis — that is frequently misattributed to lumbar disc or nerve pathology.
Overview
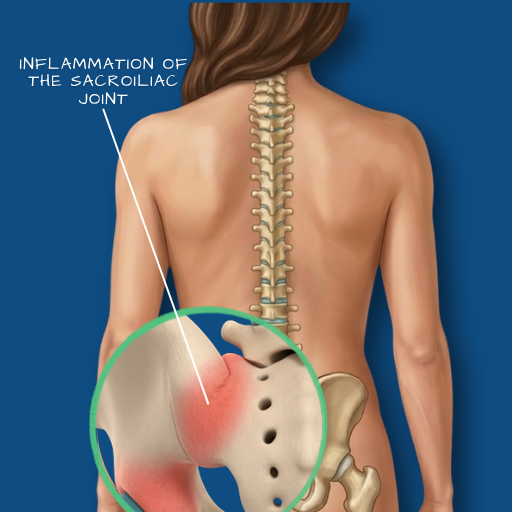
The sacroiliac (SI) joint connects the sacrum — the triangular bone at the base of the spine — to the ilium of the pelvis on each side. It is a strong, relatively immobile joint that transmits load between the spine and the lower limbs, and is stabilised by some of the strongest ligaments in the body. Despite its limited movement, the SI joint can become a significant source of low back and buttock pain when its normal mechanics are disrupted. Sacroiliac joint dysfunction is more common than is often appreciated, and it is frequently misdiagnosed — its pain pattern overlaps considerably with lumbar disc disease and hip pathology, and it does not appear on standard lumbar MRI unless specifically assessed.
Causes
SI joint dysfunction can result from trauma — a fall directly onto the buttock, a motor vehicle accident, or a significant impact that disrupts joint mechanics. Pregnancy-related hormonal changes cause increased SI joint laxity, making it a common source of posterior pelvic pain during and after pregnancy. Leg length discrepancy, prior lumbar fusion (which alters load transfer to the SI joint), inflammatory arthropathy (such as ankylosing spondylitis, which can affect the SI joints early in its course), and degenerative joint change are other recognised causes. In some patients, the dysfunction arises from altered biomechanics with no identifiable precipitating event.
Symptoms
The characteristic symptom is pain in the lower back or buttock — typically one-sided — that may radiate into the posterior thigh, groin, or outer hip. It is commonly aggravated by activities that load the joint asymmetrically: climbing stairs, standing on one leg, rolling over in bed, or sitting in a low chair. Patients sometimes describe a catching sensation in the affected buttock with certain movements. The pain is typically below the level of L5 and does not follow a dermatomal (nerve root) distribution — a feature that helps distinguish it from lumbar radiculopathy. Differentiating SI joint pain from lumbar and hip pathology requires a systematic clinical assessment — and sometimes a diagnostic injection.
Diagnosis
Clinical examination using a battery of SI joint provocation tests is the starting point — a cluster of positive tests significantly increases the probability of SI joint origin. SI joints do not appear clearly on lumbar MRI; specific SI joint imaging using CT or MRI of the pelvis is required if inflammatory arthropathy or structural damage is suspected. The most reliable diagnostic test is a fluoroscopy or ultrasound-guided SI joint injection with local anaesthetic — a significant reduction in pain following injection confirms the joint as the primary pain source. This dual diagnostic and therapeutic procedure guides subsequent management.
Conservative Care
Conservative management is the appropriate first-line approach for SI joint dysfunction. Physiotherapy addressing pelvic stability, gluteal strength, and movement pattern correction is central. A sacroiliac belt may provide short-term symptomatic support. SI joint injections with corticosteroid can provide meaningful pain relief, particularly in the acute or subacute phase. Where inflammatory arthropathy is identified, rheumatological management is co-ordinated alongside physiotherapy. Conservative management is effective for the majority of patients with SI joint dysfunction, and surgical intervention is rarely required.
Surgical Indications
Surgery for SI joint dysfunction is reserved for a small proportion of patients with confirmed SI joint pain—established through repeated diagnostic injections—who have failed prolonged, structured conservative management. SI joint fusion (minimally invasive SI joint arthrodesis) stabilises the joint and eliminates the painful movement. It is not a first-line option and is offered only after the diagnosis has been rigorously confirmed and conservative pathways have been genuinely exhausted.
Surgical Approach
Where SI joint fusion is indicated, a minimally invasive approach is used — triangular titanium implants are placed across the SI joint through a small lateral incision, under fluoroscopic or navigation guidance. The procedure stabilises the joint without the soft tissue disruption of open surgery. The Medtronic StealthStation navigation system provides the intraoperative guidance needed for accurate implant placement in what is a relatively confined anatomical corridor.
Recovery
Following minimally invasive SI joint fusion, patients are typically weight-bearing with assistance within 24 hours and discharged within two to three days. A structured physiotherapy programme begins at four to six weeks, focused on progressive loading and functional rehabilitation. Full recovery and return to unrestricted activity takes three to six months. Pain improvement following SI joint fusion, in well-selected patients, is typically significant — though as with all chronic pain interventions, outcomes are influenced by the duration of pre-operative symptoms and the accuracy of the diagnosis.
Lower back and buttock pain that has not been clearly attributed to a spinal or hip cause warrants a structured evaluation that includes the sacroiliac joint.