Vertebral Fractures
Fractures of the spinal vertebrae — from trauma, osteoporotic fragility, or pathological bone change — that require careful evaluation to determine stability, neurological risk, and the appropriate management pathway.
Overview
The vertebrae of the spine are load-bearing structures, and like all bones, they can fracture under sufficient force or when their structural integrity is compromised by underlying disease. Vertebral fractures are not a single entity — they encompass a range of injury types that differ significantly in their mechanism, stability, neurological implications, and treatment requirements. A compression fracture of a lumbar vertebra in an elderly patient with osteoporosis is clinically very different from a burst fracture sustained in a road traffic accident, and both differ from the pathological fracture seen in a vertebra affected by metastatic disease. The correct management pathway depends on identifying the fracture type, assessing its stability, and evaluating any threat to the spinal cord or nerve roots.
Causes
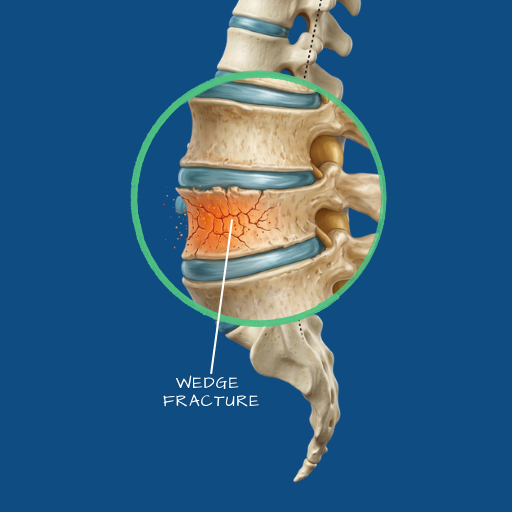
Traumatic fractures result from high-energy mechanisms — motor vehicle accidents, falls from height, sports injuries, or direct impact. They occur in structurally normal bone and range from stable compression fractures that can be managed conservatively, to unstable burst or flexion-distraction fractures that require surgical stabilisation. Osteoporotic compression fractures are the most common vertebral fracture type overall, occurring in patients with reduced bone density in response to relatively minor forces — a fall, a sudden load, or in severe cases, simply normal daily activity. They are most frequent in postmenopausal women and in elderly men. Pathological fractures occur in vertebrae weakened by tumour, infection, or metabolic disease — the fracture itself may be the presenting event that leads to the underlying diagnosis.
Symptoms
The hallmark symptom of an acute vertebral fracture is sudden onset of localised, sharp spinal pain — typically at the level of the fracture — that is worsened by movement and loading, and eased by lying down. In osteoporotic fractures, the onset may be gradual rather than acute, and some fractures are discovered incidentally on imaging obtained for other reasons. Where the fracture is associated with bone displacement into the spinal canal — as in burst fractures — neurological symptoms may be present: weakness, numbness, or in severe cases, paralysis. Any vertebral fracture with associated neurological symptoms is a surgical emergency until proven otherwise. Progressive height loss, worsening kyphosis, or a series of fractures at different levels suggests ongoing osteoporotic disease requiring metabolic assessment and treatment.
Diagnosis
Plain X-rays provide the initial assessment of vertebral height, alignment, and obvious fracture deformity. CT scanning provides the most detailed assessment of fracture morphology — the pattern of bone disruption, the degree of canal compromise, and the stability of the posterior bony arch. MRI is essential where neurological symptoms are present, where cord or nerve root compression needs to be assessed, and where bone oedema (indicating a recent or active fracture) needs to be distinguished from a chronic or healed fracture. DEXA scanning (bone density measurement) is appropriate in patients with suspected or confirmed osteoporosis. Where a pathological fracture is suspected, further workup including blood tests and whole-body imaging may be required.
Conservative Care
Stable compression fractures without neurological involvement — the most common type seen in osteoporotic patients — are typically managed conservatively. This involves a period of modified activity and pain management, followed by gradual mobilisation. Bracing may be used in selected cases to reduce pain during the acute phase. Equally important is the assessment and treatment of the underlying bone health — osteoporotic fractures are a sentinel event indicating a need for formal bone density assessment, calcium and vitamin D optimisation, and often bone-protective medication. Without addressing bone health, the risk of further fractures remains elevated.
Surgical Indications
Surgical intervention is indicated for fractures that are mechanically unstable and at risk of progressive deformity, for fractures with neurological compromise requiring decompression, for fractures that have failed conservative management with persistent severe pain, and for selected osteoporotic compression fractures where minimally invasive cement augmentation is appropriate. Pathological fractures may require surgery for stabilisation and, in some cases, to obtain tissue for diagnosis.
Surgical Approach
For osteoporotic compression fractures causing persistent pain without neurological compromise, vertebroplasty or kyphoplasty—minimally invasive procedures in which bone cement is injected into the fractured vertebra to stabilise it and restore some height—can provide rapid pain relief. Kyphoplasty uses a balloon to create a cavity before cement injection, offering greater height restoration. For traumatic burst fractures or unstable fractures with neurological compromise, open surgery to decompress the spinal canal and stabilise the injured segment with pedicle screws and rods is required. The Medtronic StealthStation navigation system is used in stabilisation procedures to guide instrumentation accurately in anatomy that is often distorted by the fracture itself.
Recovery
Recovery varies significantly by fracture type and treatment. Following vertebroplasty or kyphoplasty, patients are typically mobile within hours and experience meaningful pain relief within days. Hospital stay is usually one to two days. Following open stabilisation surgery for traumatic fractures, recovery follows a similar trajectory to fusion surgery — five to seven days in hospital, structured activity restrictions, and a rehabilitation programme over three to six months. Neurological recovery, where it occurs after spinal cord or nerve root decompression, progresses over months and is not always complete — the extent of recovery depends on the severity and duration of the original injury.
Any sudden onset of severe spinal pain following a fall, impact, or physical stress should be evaluated promptly.