Spondylolisthesis
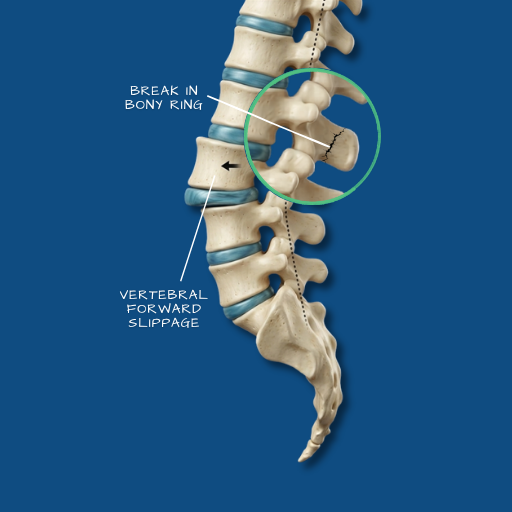
A condition in which one vertebra slips forward over the vertebra below it, affecting spinal stability and potentially compressing nerve roots in the process.
Overview
The vertebrae of the spine are stacked in a column and held in alignment by discs, ligaments, and facet joints. Spondylolisthesis occurs when this alignment is disrupted and one vertebra slides forward relative to the one below it. The degree of slippage is graded from I to IV — from mild (less than 25% displacement) to severe (greater than 75%). Most clinically significant cases fall in the Grade I or II range. The lumbar spine, particularly the L4–L5 and L5–S1 levels, is most commonly affected. Depending on the degree of slippage and whether nerve compression is involved, spondylolisthesis may be asymptomatic, a source of chronic low back pain, or a cause of significant nerve-related symptoms.
Causes
The causes of spondylolisthesis vary by patient age and type. Degenerative spondylolisthesis — the most common form in adults over 50 — results from age-related breakdown of the disc and facet joints that normally prevent vertebral movement. As these stabilising structures weaken, the vertebra begins to shift forward. Isthmic spondylolisthesis, more often seen in younger patients and athletes, results from a stress fracture in a specific part of the vertebra (the pars interarticularis) that allows forward movement to occur. It is particularly associated with activities involving repeated spinal extension — gymnastics, cricket fast bowling, weightlifting. Less commonly, spondylolisthesis results from traumatic injury or from pathological bone changes.
Symptoms
Low back pain is the most consistent symptom — often described as a deep, central ache that may worsen with prolonged standing, walking, or activity that loads the lumbar spine. In cases where the slippage compresses nerve roots, radiating leg pain, numbness, or weakness may also be present — similar in character to sciatica. Some patients notice a visible step deformity at the lower back, or a change in posture — an increased lumbar curve or forward pelvic tilt — as the body adapts to the altered spinal alignment. In higher-grade slippages, gait changes and difficulty standing upright may be apparent. Red flags — rapid neurological deterioration, loss of bladder or bowel function — require urgent assessment.
Diagnosis
Standing lumbar X-rays are the initial and often most informative imaging study, as they capture the dynamic alignment of the spine under load — something an MRI taken lying down does not fully reflect. Flexion-extension X-rays (taken with the patient bending forward and backward) can reveal instability — movement between vertebrae that indicates the slip is mobile rather than fixed. MRI provides detail on disc health, nerve compression, and the condition of the facet joints. Together, these imaging studies guide both the diagnosis and the treatment decision.
Conservative Care
Many patients with low-grade spondylolisthesis are managed effectively without surgery. Physiotherapy targeting lumbar stabilisation — strengthening the deep abdominal and paraspinal muscles that support the affected segment — is the foundation of conservative management. Activity modification, particularly avoiding extension-loading movements in symptomatic isthmic cases, is important. Anti-inflammatory medications and, where appropriate, epidural or facet joint injections can provide symptomatic relief. Conservative management is the appropriate starting point for most Grade I and Grade II cases, and for patients without significant neurological involvement.
Surgical Indications
Surgery is considered when conservative care has not produced adequate relief over an appropriate trial period, when the slip is progressive (increasing in grade over time), when neurological symptoms are present and not improving, or when the patient’s functional limitations are significant. The combination of instability and nerve compression — common in higher-grade slippages — is a clear indication that conservative management alone is unlikely to provide a durable solution.
Surgical Approach
The standard surgical approach for spondylolisthesis requiring intervention is spinal fusion — stabilising the affected segment to prevent further movement and, where appropriate, reducing the degree of slippage. This is typically performed as a posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF), in which the disc is removed, a cage is placed in the disc space to restore height and alignment, and pedicle screws are used to stabilise the vertebrae. The Medtronic StealthStation navigation system is used routinely in these procedures to guide accurate pedicle screw placement and reduce the risk of positional complications. Where possible, a minimally invasive approach is used to reduce soft tissue disruption and support a more manageable recovery.
Recovery
Recovery from spinal fusion for spondylolisthesis is more gradual than from decompression-only procedures. Patients are typically mobile within 24–48 hours of surgery and discharged within three to five days. The early recovery period — the first six weeks — involves structured restrictions on lifting, bending, and twisting while the fusion begins to consolidate. Physiotherapy begins once early healing has occurred and focuses on building the strength and movement control needed to support the fused segment. Return to desk work is generally possible within six to eight weeks. Return to physical activity and sport takes longer — three to six months or more — and is guided by both clinical progress and imaging confirmation of fusion.
If you have been told you have spondylolisthesis, or if these symptoms reflect your experience, a consultation will clarify the grade, the stability, and the appropriate management pathway.