Disc Herniation
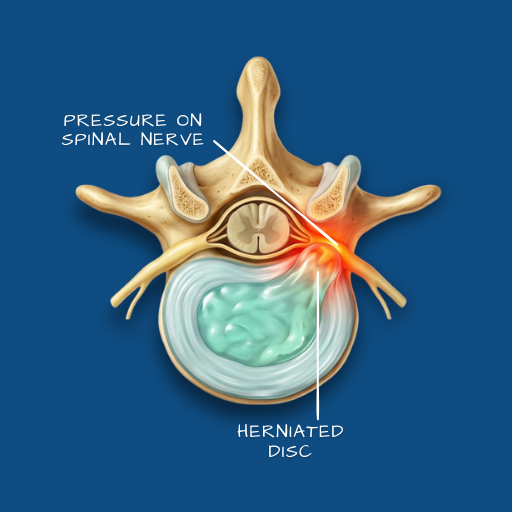
When spinal disc material presses on a nearby nerve root, causing pain, numbness, or weakness in the back, neck, or limbs.
Overview
The spine is supported by intervertebral discs — circular structures made of a tough outer ring and a gel-like inner core. A disc herniation occurs when the inner material pushes through a tear or weakness in the outer ring and comes into contact with an adjacent nerve root. This pressure is what produces most of the symptoms the patient experiences. Disc herniations are most common in the lumbar spine (lower back) and the cervical spine (neck), and they affect people across a wide age range — though they are particularly common in working-age adults. Left unmanaged, the pressure on the nerve can lead to progressive weakness in the affected limb.
Causes
Disc herniations typically result from a combination of structural wear and mechanical stress. With age, discs lose water content and become less resilient — a process that makes them more susceptible to tearing under load. A sudden increase in spinal pressure — from lifting, twisting, or a fall — can trigger herniation in a disc that has already begun to degenerate. In younger patients, herniations often follow significant physical activity or trauma. In older patients, they may occur with minimal provocation. Occupation and lifestyle are contributing factors: prolonged sitting, repetitive bending, and heavy manual work all place cumulative load on the lumbar discs.
Symptoms
The most common presentation is pain that radiates from the spine into a limb — down the leg in lumbar herniations, or into the arm in cervical cases. This radiating pain is often described as sharp, burning, or electric in character, and is typically made worse by sitting, bending forward, or coughing. Numbness and tingling in the affected limb are also common. In more significant herniations, the patient may notice weakness — difficulty lifting the foot, gripping objects, or climbing stairs. Red flags requiring urgent attention include loss of bladder or bowel control, rapid progression of weakness in both legs, or saddle area numbness — these indicate possible cauda equina syndrome and require immediate evaluation.
Diagnosis
Clinical examination — including neurological testing of reflexes, sensation, and motor strength — provides the initial picture. An MRI of the affected spinal segment is the imaging of choice, as it shows the soft tissue structures, the disc, and the degree of nerve compression in detail. A CT scan may be used where MRI is contraindicated or where bony detail is specifically required. X-rays alone are insufficient for diagnosing disc herniation, as they do not show soft tissue, but they remain useful for assessing spinal alignment.
Conservative Care
The majority of disc herniations resolve or improve with structured conservative management, without requiring surgery. Physiotherapy is the cornerstone of this approach — targeted exercises to relieve nerve pressure, strengthen the supporting musculature, and restore functional movement. Pain management, including anti-inflammatory medications and in some cases nerve block injections, can make physiotherapy more accessible during acute flare-ups. Activity modification — avoiding the specific movements and positions that aggravate symptoms — is equally important. Conservative care is typically trialled for six to twelve weeks before a surgical conversation is considered, provided there is no neurological deterioration during that period.
Surgical Indications
Surgery becomes the appropriate consideration when conservative care has been adequately trialled without sufficient improvement, when the patient’s quality of life is significantly and persistently impaired, or when there is evidence of neurological compromise — weakness, progressive numbness, or the red flag symptoms described above. The goal of surgery is not to cure the disc but to relieve the pressure the disc is placing on the nerve.
Surgical Approach
For lumbar disc herniations, the procedure most commonly used is a microdiscectomy — a minimally invasive operation in which the herniated disc material is removed through a small incision, using magnification to preserve surrounding tissue. The Medtronic StealthStation navigation system is used where anatomical complexity or prior spinal history warrants additional intraoperative guidance. The aim is to decompress the affected nerve with the smallest necessary intervention, preserving as much of the disc and surrounding structure as possible. Cervical disc herniations may be addressed through an anterior cervical discectomy and fusion or cervical disc replacement, depending on the clinical picture.
Recovery
Following microdiscectomy, most patients are mobile within 24 hours and discharged within two to three days. The initial weeks involve activity restriction — avoiding heavy lifting, prolonged sitting, and bending — while the nerve recovers. Physiotherapy typically begins within two to four weeks of surgery and plays an important role in restoring strength and movement patterns. Return to desk work is generally possible within four to six weeks. Return to manual or physical work, and to sport, takes longer — typically three to six months, depending on the demands of the activity and the pace of individual recovery. Nerve symptoms — numbness, tingling — may persist for weeks to months after the pressure has been relieved, as nerve recovery is inherently slow.